10 Tips that Everyone Should Know Before Performing an Implant Treatment in the aesthetic zone


Table of Contents
Introduction
Nowadays, implantology is a predictable area and well-accepted by the scientific community for missing or doubtful prognosis tooth repositioning.
More than 30 years ago, Brånemark published the first articles presenting implantology as a safe and predictable method to rehabilitate edentulous patients.
One of the key factors was the time the implant was submerged until loadin- 3 months for the jaw and 6 months to the maxilla (Bränemark 1977).
Years later, Albrektsson establishes success criteria for every treatment involving implants, where implants should be absent of mobility, pain, radiolucency around the implant, and the bone loss should never bee than 1,5 mm and 0,2 mm per year (Albrektsson 1986).
Although, this is a prevailing criteria, at that time treatments involving implants was mainly functional.
Nowadays we know that our patients are quite demanding regarding aesthetic results.
Three years later, Smith published that aesthtics have also an important role in successful implant treatment (Smith 1989).
For that there are some golden rules that every implantologist should manage to achieve predictable results in the aesthetic zone, and this article there will be described ten rules that everyone should consider:
1) The edentulous gap in the aesthetic zone: When will there be papilla?
The presence of papilla between an implant and teeth depends mainly on the presence of interproximal bone peaks in the adjancent tooths.
If there is not bone peaks, there will not be papilla (Kan 2003).
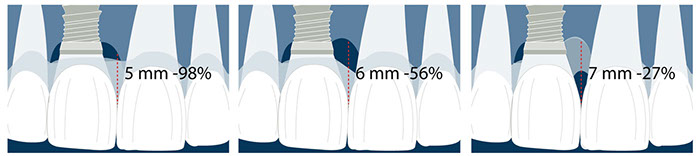
There is also a relation between the presence of the papilla and the distance between the contact point and the bone crest (Tarnow 1992).
There will be a high likelihood of complete presence of papilla if this distance is 5mm or less.
This probability goes down for 6 mm (56%) and 7 mm (27%) of distance.
Although the trial was performed in natural tooth, Salama (Salama 1998) and co-workers found that 4,5 mm of papilla was the average amount of papilla that we should expect to have between an implant and tooth if a distance of at least 1,5 mm was maintained between an implant and tooth.
Also read more about Tarnow's article in this publication about how we should have our own criteria regarding scientific publications.
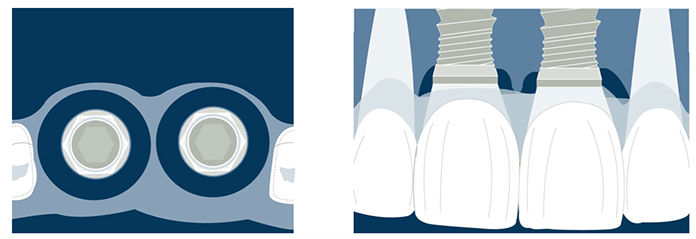
2) Placing two adjacent implants in the aesthetic zone. What should we expect?
Placing two implants adjacent is always a big challenge.
The mean papillary height between implants will be 3,4 mm, which is in, most cases, insufficient to achieve an optimal aesthetic result (Tarnow 2003).
This issue can be solved by placing one implant to replace two anterior missing tooths.
This way it is expected to achieve a higher papilla level between an implant and a pontic (5,5mm) (Salama 1998).
3) Selecting the correct abutment.
It is essential to choose the right abutment when we are performing an implant supported restoration in the aesthetic zone.
If there is a thin mucosa with less than 2 mm width, zirconia is the best options cause metallic abutments will show a color alteration of the peri-implant soft tissue (Jung 2007, 2008).

4) Immediate implants and aesthetic results. What should we know?
Althought it is a very discussed topic; there is some basic knowledge about immediate implants in the aesthetic zone.
Unavoidable bone resorption happens when a tooth is extracted (Cardaropoli 2003, Schropp 2003, Araujo & Lindhe 2005).
These events are not avoidable if the implant is placed during the extraction (Botticelli 2004, Araujo & Lindhe 2006).
Some protocols are published to correct this event, like performing a connective tissue graft at the time of the immediate implant (Kan 2000), but the recession of the gingival margin is likely to occur (Evans 2007).
This facial recession will be more pronounced in a thin biotype rather than a thick biotype (Kan 2011), so there could be stated that immediate implants in a thin biotype are not predictable.
Delayed implant treatment and other treatment options should be considered, like ridge preservation (Jung 2012).
The ITI guide is also an amazing book to start learning more about immediate implants.

5) Early Implant placement. A predictable alternative.
The timing when the implant is placed is also a huge topic (Hämmerle 2004).
One option is to perform the extraction and after, one month, place the implant with simultaneous ridge augmentation (Buser 2013)—this method has been proven to be a reliable way to achieve predictable aesthetic results.
This technique almost always involves some guided bone regeneration.
6) Provisional restoration. Is it mandatory?
After extraction of the teeth, it is essential to preserve the papilla architecture.
Therefore, some authors stated that placing an implant while the teeth are extracted somehow helps maintain the shape and the papillary architecture.
Even if there is no provisional after the surgery, it is essential to reshape the soft tissue before placing the definitive prosthesis.
Therefore, the temporary restoration is also a way to achieve the final peri-implant shape and transfer this emergence profile to the lab (Elian 2007).
Some of these contents are well explained in this ebook about immediate loading.



Fig. 12-13-14: Every demanding aesthetic treatment involving implants should have a provisional phase before the definitive prosthesis is delivered. It is mandatory to design natural emergence profiles before finishing the treatment.
7) Managing provisionals in implants in the aesthetic zone. Current concepts.
During the provisional phase of the treatment, a correct and natural emergence profile should be created following the adjacent tooth.
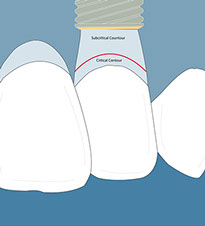
In every emergence profile, two contours can be differentiated (Su 2010):
- Critical contour: The contour is 1 mm immediately below the gingival margin. This contour, when modified, can displace the gingival margin apically.
- Subcritical contour: This is the contour below the critical contour.
When properly managed, this contour can create soft tissue volume (concave); once this volume is created, it can be displaced where needed.
There are other ways to manage the provisionals during the healing phase, but always regarding the concepts posted before (Wittneben 2013).
Provisional play a key role in mantaining soft tissue around implants in the aesthtic zone and should always be used.
8) Implant three-dimensional position. Where to place the implant
If an implant is placed in the anterior aesthetic zone, some rules should be a guide for every implant placement (Buser 2004):
Medio distally: The implant should be at a distance of 1,5 mm from the adjacent teeth.
This is the minimal distance, although some articles even showed that 2 mm would be an improvement (Gastaldo 2004).
Apico-coronally: This distance should be 3-4 mm from the gingival margin of the future restoration. In immediate implants, the reference is the gingival distance of the removed teeth. If there were no tooth previously, a wax-up should create a reference to the future restoration.
Buccal-palatal: The buccal part of the implant should be 1-2 mm palatal to the emergence profile of the adjacent teeth.



Fig.16, 17, 18- Placing the implant in the comfort zone is a requisite when implants are placed in the aesthetic area.
9) Choosing the right implant.
There is an increasing implant market in almost all countries with some new implant brands.
Of course, this is something positive for the clinician, but we must be well aware of the different implant companies that can fulfill our expectations and the treatment and patient goals.
Platform switching is a biological concept well implemented in almost all implant brands (Lazzara 2006).
Still, we should know that although it is an important issue, platform switching is not the only factor that can contribute to less bone remodeling after implant placement.
Lately, Zipprich (Zipprich 2007) proved that the stability between the implant and the abutment is crucial to avoid the “pumping effect,” which leads to bone resorption.

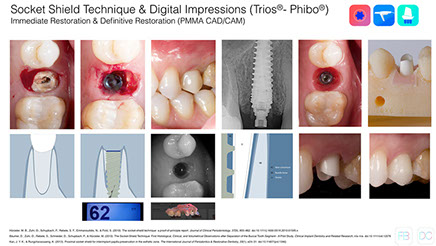
10) New techniques to avoid buccal bone resorption.
Several methods have been described to avoid the negative effect of extraction like immediate implants (Botticelli 2004, Araujo & Lindhe 2006), and barrier membranes (Lekovic 1997).
However, ridge preservation is the most suitable technique for preserving the socket's volume (Araujo 2009).
Lately, a new technique is described as an option to perform an immediate implant without the negative consequences of bone remodeling after an extraction (Hürzeler 2010).
The rationale behind this technique is preserving a tooth fragment that will avoid resorption after the extraction.
Although this technique is quite promising, we should be aware of the incoming publications about a more extensive follow-up and the predictability of leaving a fragment inside the socket after an extraction (Baumer 2013, Kan 2013).
Conclusions
Today we can find in the literature an essential number of reliable protocols to achieve satisfactory aesthetic results in our treatments.
But we should consider that success is most likely if a correct diagnosis and treatment plan is carried out.
We should use some essential tools daily in our daily practice to assess and help the clinician identify the complexity of a case before a treatment plan is defined (Buser 2009).
Clinicians should also perform protocols well described in the literature and with a follow-up that categorizes that treatment option as predictable in the long term.
Nowadays, there is sufficient data and scientific background to establish clear guidelines when demanding aesthetic treatments involving implants are required.
Check Your Knowledge
Comments
0 totalLoading comments...
Previous
Bio-Oss® Collagen in the Buccal Gap after an Inmediate Implant
Next
Platform Switching. A Biological Concept
Related Articles

Dental KOL Marketing: How Implant and Periodontal Brands Build Their Key Opinion Leader Bench
11 min read
Dental Video Marketing: How Brands Use Clinical Video to Drive KOL Adoption
12 min read