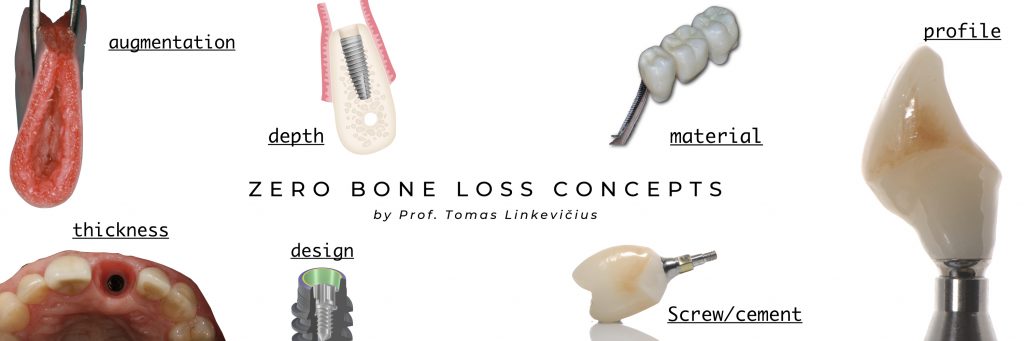
Zero bone loss concepts by prof. Tomas Linkevičius. A path to crestal bone stability

Table of Contents
Crestal bone stability around dental implants remains one of the most important and wanted features of successful implant treatment. Yet, it seems like crestal bone loss was with us forever, and that really for the majority of clinicians became a norm.
Maybe that’s because we all have been taught by Albrektsson and co-authors study published in 1986, that 1.5 mm of bone loss within the first year of loading can be considered as a success if a later bone loss does not exceed 0.2 mm annually. There are so many possible reasons for bone loss, that dentists think that it is not possible to control all of them, and tend to give up the idea of crestal bone stability.
However, I consider this kind of approach outdated and I refuse to accept the idea that bone loss is unavoidable. That was why, with my research team, we have developed Zero bone loss concepts – clear clinical protocols, meant to develop and maintain crestal bone stability around implants.
Besides major clinical advantages to the patient, stable marginal bone provides us, the clinicians, with psychological comfort and satisfaction, because of positive long-term outcomes.
We would like that all our cases would look like that
Therefore we all need to be aware of possible causes, which can lead to loss of crestal bone stability and exercise every method to prevent bone resorption.
But before we try to emphasize the reasons for bone loss, let’s look into why bone resorption is so damaging to implants. At least 3 major problems can occur in the long term.
Why accepting initial bone loss after 1 year?
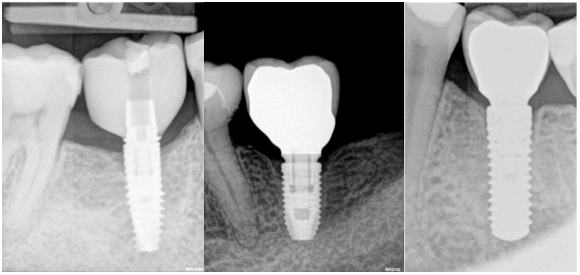
First, clinicians tend to accept initial bone loss after 1 year, as usually bone loss does not progress, however, even if cone levels remain status quo, still there is a substantial threat, that it might lead to significant peri-implantitis, once re-infected.
We must be aware, that predictable peri-implantitis treatment is still to be developed, thus the best treatment would be prevention, in my opinion.
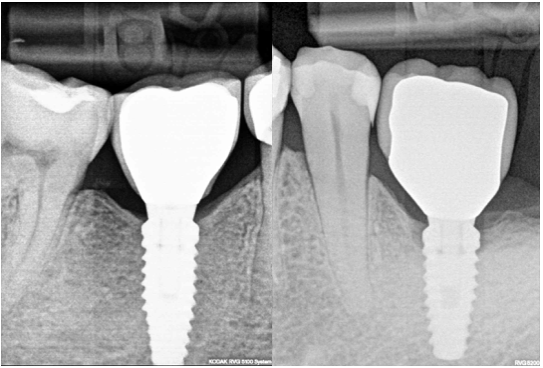
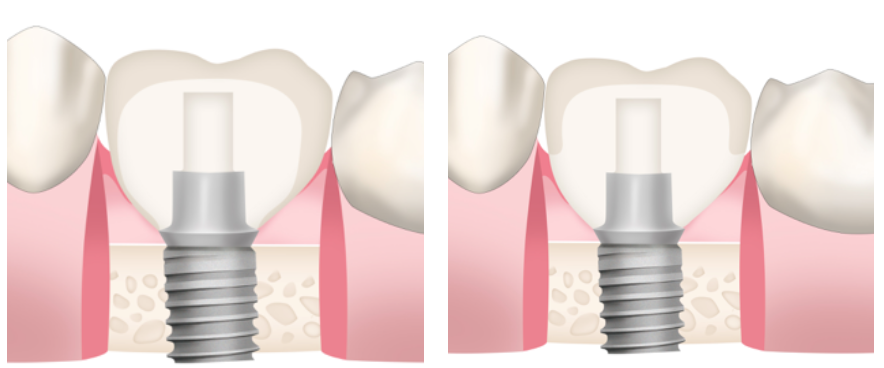
On the other hand, let’s admit, that all of us would choose Fig 1 A implant, without bone loss, and not Fig 1B implant, although the difference is very small. Sometimes clinicians tend to downplay this bone loss because simply they do not understand, why the bone is disappearing, and are not eager to learn.
Bone loss and short implants. A dramatic relationship
Secondly, crestal bone stability is especially important for short implants, which usage is becoming common practice. Today, an 8 mm long implant is not considered as short anymore, and we have sufficient data to say, that 6 mm long implants work as good as longer ones in posterior areas of both jaws.
However, imagine, what will happen, if a 6 mm implant is placed in the mandibular posterior jaw region, where thin vertical soft tissues are frequently present? We would have approximately 2 mm of bone resorption, due to biological width formation. It leaves only 2/3 of implant surface osseointegrated. Now, that is a real threat for the implant to fail, having in mind prosthetic suprastructure and implant/crown ratio.
Some implant manufacturers have launched 4 mm length implants, therefore soft tissue thickness is even more important for the users of these products.
Height of the underlining bone
Finally, it is important that the stability of peri-implant mucosa level around the implant is largely dependent on the height of the underlying bone.
The consequence of marginal peri-implant mucosa migration, as a result of early marginal bone loss, has a major implication in the aesthetics of the restoration, particularly in the anterior area.

So which factors are important to keep bone stable, and prevent mentioned complications?
Almost for one-decade platform switching was considered to be the most effective way to achieve this task. It was so effective that almost all implant companies have implemented platform switching as a “must be” feature of implant manufacturing.
Everybody made the conclusion that implant design was more important than the biology itself. However, recent clinical research of our group has shown that soft tissue thickness is an important factor in preserving crestal bone stability around implants.
It was determined that if vertical soft tissue thickness is 2 mm or less, there will be crestal bone resorption of 1.5 mm extent during the formation of a biological seal between soft tissues and implant/abutment/restoration surfaces.
Further research of our team has shown that the minimum height of soft tissues should be 3 mm to avoid bone loss, while 4 mm being optimal number, as it also allows better development of a prosthetic profile of the restoration.

Furthermore, it was clearly shown that even implants with platform switching modification couldn’t maintain bone if, at the time of implant placement, vertical soft tissues were thin.
That brings the discussion – what is more important, biology or implant design back on the table. Well, to continue further, we need to understand, that vertical soft tissue thickness is the prerequisite of the biological width around implants.
Biological width around implants starts to form at the time of healing abutment connection and is completely finished after 8 weeks. This biological seal is the only and most important protection barrier of the osseointegrated implant from the contaminated intraoral environment.
Thus there is a direct connection between pre-implant mucosa of the edentulous alveolar ridge and peri-implant soft tissues. It seems that soft tissue thickness required to protect underlying bone around implants is approximately 4 mm, which is longer, compared to biological width around teeth.
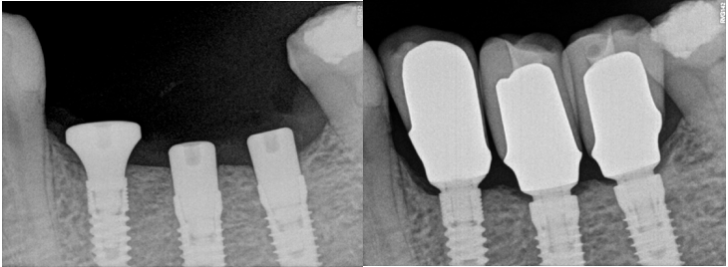
There are 2 ways how biological width around implants can be formed:
With crestal bone loss or without bone resorption.
Which one would you like to your patient to have?
Or which one would you like your mother to have? That’s the question we all as clinicians should answer sincerely.
So if we diagnose thin vertical tissues at the time of implant placement, what should we do? To answer this need, we have created the guidelines to follow because we will have crestal bone resorbtion otherwise.
So what is the strategy? There are several options, some of them already researched clinically; some of them are based on clinical expertise.
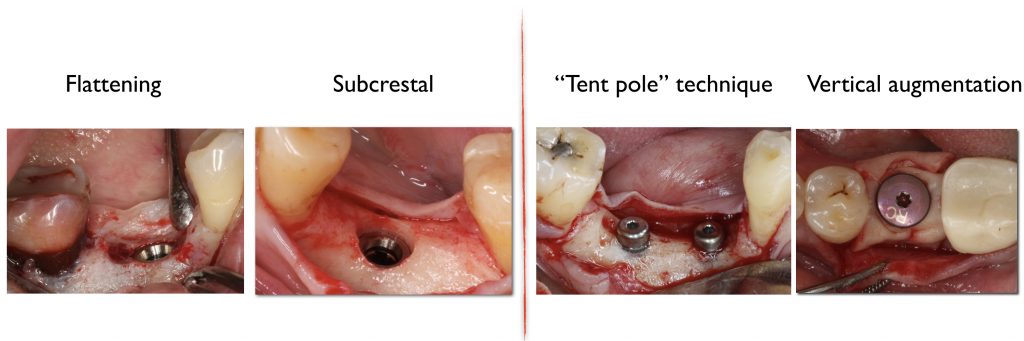
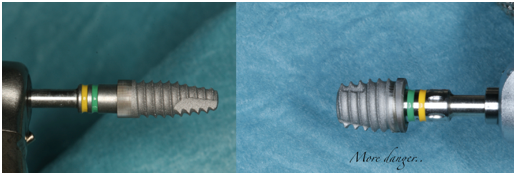
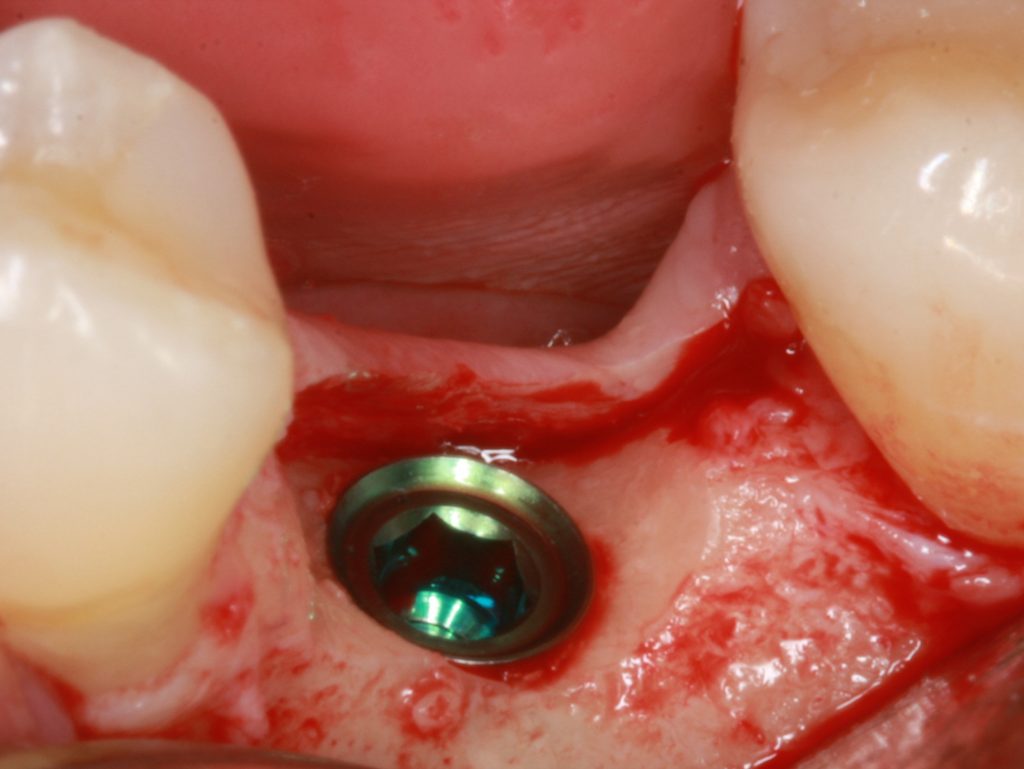
The first thought, which enters the mind, just places implant deeper subcrestally (Fig 5). Firstly, there must be enough place for the alveolar nerve that the implant could be positioned subcrestally in a safe manner.
It is advised that the implant would stop at least 1 mm over the nerve. Subcrestal placement is suggested to cause controlled bone remodeling, but not a bone loss. It is interesting to note, that not all implants can be placed subcrestally. In addition, implant-abutment connection stability becomes very important, if located subcrestally.
Another option might be recontouring of the bone during basic implant bed preparation, especially if narrow ridge is present.
Careful reduction and smoothening of the narrow ridge not only will provide a flat bone surface and a sufficiently wide area of bone for implant positioning, but would increase soft tissue thickness as well.
Again, “the removal of the bone to preserve the bone” concept might not acceptable to some clinicians, nonetheless that there is no strong clinical evidence suggesting this procedure to increase soft tissue thickness and reducing crestal bone remodeling.
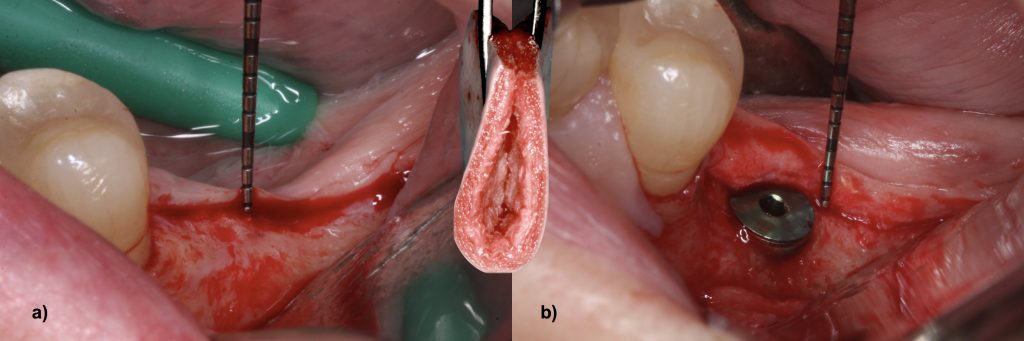
Consequently, we might think in other direction and use the third option – vertical reconstruction of soft tissue thickness, which in my opinion is the most logical one. Increasing soft tissue thickness vertically compensates the lack of vertical tissue thickness.
Already in JOMI 2009 paper “The influence of soft tissue thickness on crestal bone changes around implants: a 1-year prospective controlled clinical trial” we have suggested to “…to consider the thickening of thin mucosa before implant placement”, therefore this concept is not entirely new.
The idea is to place some sort of autogenic, allogenic, or xenogeneic material over the implant in that way increasing soft tissue thickness after healing.
A connective tissue graft is considered as the golden standard for soft tissue augmentation around implants. However, this technique has some serious disadvantages, like donor site morbidity and the difficulty of the harvesting procedure.
Therefore soft tissue substitutes might be considered as a viable option to replace autogenous grafts in vertical soft tissue reconstruction.
A series of studies prove that the lack of vertical soft tissue thickness required for biological width formation without crestal bone loss can be compensated by the use of acellular dermal matrix material at the time of implant placement.
Zero bone loss concepts’ prosthetic factors include screw-retained restorations, titanium bases with high gingival parameter, and polished zirconia in subgingival space to develop epithelial adherence.
Zirconium as a material is considered the best for peri-implant soft tissues. However, it’s evident that it must be treated in a special manner – to be polished enough.
So the polishing must be provided. It’s important not to make “Zr without Zr” restorations when veneering porcelain covers Zr and does not allow direct contact between soft tissues and zirconium. In that way, the biocompatibility effect might be reduced.
One important take home message is, that there is no the most important factor to ensure crestal bone stability. It is the combination and interaction of factors that determine the outcome.
It is only through accepting this multifactorial reality that clinicians can change their thinking and begin on the path to zero bone loss.
This path consists of 4 levels:
(1) scientific articles;
(2) the book;
(3) Online course; and
(4) Live course.
Each level will bring you closer to the goal – stability of crestal bone around your implants.
The unique situation of the current Covid-19 epidemic created a situation, where demand for online education became very obvious.
Therefore, we have moved our live 2-day course with hands-on to the internet and created Zero bone loss concepts Online!
Recommended Book
Related Reading: Understanding crestal bone stability starts before implant placement. If you want to optimize ridge dimensions before surgery, our guide on socket preservation and alveolar ridge preservation techniques covers the evidence-based protocols for maintaining bone volume after extraction.
Zero Bone Loss Concept Book

Comments
0 totalLoading comments...
Previous
Periospot´s Bookshelf: April 2020
Next
4 Techniques to Perform an Effective Ridge Preservation and Soft Tissue Management
Related Articles

Machine Learning for Dentists: Predicting Implant Success with AI
1 min read
Osseointegration: The Stuff That Actually Makes Dental Implants Work (And Why You Should Care)
13 min read