5 Concepts to Achieve a Successful Immediate Implant Placement Into a Fresh Molar


Table of Contents
The fact that you’re spending your precious time reading these lines right now is mind-blowing. Seriously. And as an act of appreciation we are not going to waste your time, so let’s get started.
A while ago I posted a clinical case on Facebook. An upper first molar's immediate implant.
My friends started to drop comments and, as usual in every cases, fired an healthy discussion with almost all the participants agreeing with the approach.
However, a good friend of mine posted the following comment:
“ Dude, waiting 3 months is much more easy...”

At first I thought: “He´s right, maybe performing the extraction and waiting for 3 months would have been a more predictable and technically simpler approach”.
His remark caught my attention. He wasn't wrong. But then, after spinning around the matter, I thought: ”Well, the literature is on my side and for having preformed an immediate implant I decreased roughly 3 months the global treatment time, which in this case was crutial since the patient was having his daughters wedding in about 5 months. But the most important thing was this big barbecue party with his friends. Options!
Coincidently, before I started the treatment I gave the patient 2 options:
1) Extract, perform an alveolar ridge preservation, wait 3-4 months, place the implant and after 10 weeks place the definitive restoration: Global treatment time - nearly 6 months.
2) Extract, place the implant the same day and after 3 months place the definitive restoration: Global treatment time - 3 months.
As a clever business man, my patient asked:
-“But is the option 2 as reliable as the option 1?”
Answer:
- “Statistically and based on the scientific background: definitely YES (W. Becker & B. E. Becker 1995; Schwartz-Arad et al. 2000; Fugazzotto 2008; Cafiero et al. 2008)
My patient accepted the treatment involving immediate placement. The previewed timeline was respected and after 4 months he was happy with his new molar, ready to function in his daughter’s wedding banquet.
But regarding our daily practice, which concepts should we manage to achieve a successful treatment outcome? Let´s go through it right now:
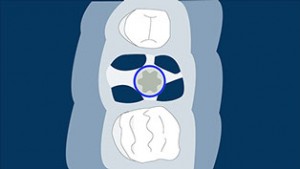
#1 The Site Classification
There are three type of sites that will help us to make decision about which approach should we consider to place (or not to place) the implant (Smith & Tarnow 2013).
Type A socket: This kind of socket has enough septal bone to surround the entire implant and the primary stability is entirely supplied by the septum.
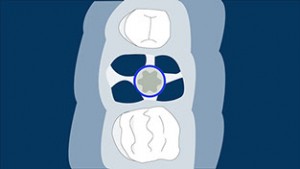
Type B socket: The septal bone will partially surround the implant, enough to achieve a minimal torque value, although sometimes the implant has to be placed slightly apically (3-5 mm) in order to achieve primary stability (Schwartz-Arad & Chaushu 1997a).
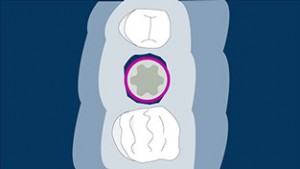
Type C Socket: In this type of sockets the shape of the site is similar to an hourglass where the thickened area corresponds to the furcation. The problem of placing immediate implants in this type of site is that you have to engage your implant (really wide implant. 7-9 mm wide) to the buccal and lingual walls which if not performed properly is very likely to undergo into a bone resorption. This kind of sockets in my experience are a “no-bet” for me, and I only play the odds here if I can get primary stability apically to the socket.
I also loved the way José Navarro presented here this topic at FOR page.
Watch the webinar here
https://youtu.be/dpcyyscCzws
#2 Primary stability
What a nice and controversial topic here. Some authors described that the minimal implant torque value (ITV) should be 15 N·cm and with this torque the expected survival rate will be around 86%, although when that implant minimal torque value is greater than 30 N·cm the survival rate will increase to 90% (Walker et al. 2011). But let’s get serious with this. Torque does not always tell us the truth and that’s why we have other ways to get more information on what is really happening down there when an implant is placed. I´m really an Osstell advocate.
Whenever I doubt the survival probability of an implant that I just placed, I pick up my Osstell and I control the ISQ evolution of that implant by measuring the ISQ values during the healing time.
If we combine a good implant torque with an acceptable ISQ value, where you’d want to have a torque value over 30 N·cm and an ISQ value above 60, our implant is very likely to be successful (Block 2011). (in another article I’ll give you the rational on this topic - Osstell and Torque values) #3 Anatomical Limitations As you know, in the upper jaw the major limitation is the sinus, and in the lower jaw the dental nerve is more than a limitation, is an untouchable structure.
Does this mean that if the sinus is close to the remaining site after the molar extraction, I will not be able to perform an immediate implant in the upper jaw? The answer is NO! It is described in the literature how an immediate implant in a molar site can be performed simultaneously to a sinus floor augmentation via osteotomes (Artzi et al. 2003).
You can see a full case here performed by Daniel Rodrigo. This guy is just amazing. Unfortunately that option cannot be performed in the lower jaw, because inferior alveolar nerve lateralization cannot be justified to allow an immediate implant.
#4 The remaining gap. What should I do with it?
This topic could be the responsible for the next World War III. Some authors are advocates of not filling the gap with nothing more than the blood clot (Schwartz-Arad & Chaushu 1997b; Wöhrle 1998; Tarnow & Chu 2011), and others state that in some conditions gaps should be filled with some bone substitute if the gap is superior to 2 mm (Akimoto et al. 1999; Wilson et al. 1998). Since we are going to perform a flapless approach, we should consider always filling the buccal gap, as it could help to preserve the dimensions of the ridge (Araújo et al. 2011).
#5 Finally: When not to perform an immediate implant
We all use “To-Do” lists, and we love them. I my self I´m an Evernote and Wunderlist advocate. It helps to keep me organized and disciplined. But sometimes I think that even more important than having a “To-Do” list, is having a “Not-To-Do” list. Why? It can save us a lot of problems. Let´s be clear here: if some or all the buccal wall is missing, don´t try to be a hero (your patients don´t need a hero, they just need a dentist) and just do a staged approach- Regenerate and then do a delayed implant placement, like my pal said on my post on Facebook. Add this to your "Not-To-Do" list.
There’s a catch: It is possible that you may have to perform a guided bone regeneration after the healing time, if a severe bone remodeling occurs during the healing period.

#6 Extra Bonus: An animation to show you the correct implant placement
Creating illustrations and animations really gives me a lot of work, but I feel happy when readers give me their positive feedback. This feedback is even more important when it is about improving or refining, in a small part or a whole, allowing me to provide a proper understanding of what that animation is trying to explain. That´s why this Saturday morning I decided to create this extra content where it is explain how deep your implant should be placed and why is so important to have a correct emergence profile. Hope you enjoy it (if you don´t… don´t complain cause it took me almost 2 hours to finish it).
Conclusion
If I had to pick just one article which supports that immediate implants after molar extractions is a safe and a reliable article I would choose the Fugazzotto article. It has a great follow up and the number of subjects that were included in the trial is quite considerable (386 patients).
Following the conclusions that can be found in the literature about this topic, we can state that immediate implants at fresh molar sites is a reliable and predictable treatment if it is performed following some of the simple rules explained above.
I hope you enjoyed this article as much as we enjoyed writing it so subscribe to our newsletter to stay tuned and write us if you would like to collaborate with our program.
Comments
0 totalLoading comments...
Previous
4 connective tissue harvesting techniques that may help you in your daily practice
Next
Bio-Oss® Collagen in the Buccal Gap after an Inmediate Implant
Related Articles

Machine Learning for Dentists: Predicting Implant Success with AI
1 min read
Osseointegration: The Stuff That Actually Makes Dental Implants Work (And Why You Should Care)
13 min read